Pleurodesis technique with intrathoracic, hyperthermic chemotherapy
(The text is taken from the doctoral thesis of Dr Athanasios Kleontas)
After a complete clinical-laboratory, preoperative examination, the patient is taken to the operating room with the chest drainage tube already in place.
After connecting the necessary epidermal sensors and electrodes for the complete and continuous recording of the patient's vital signs and cardiorespiratory function, the patient is introduced under anaesthesia and intubated with a double lumen tracheal tube. Confirmation of good tracheal tube function, with satisfactory lung blockage of the affected hemithorax. Maintenance of anaesthesia with intravenous anaesthetic drugs and maintenance of muscle relaxation. Insertion of a triple line, a central venous catheter in the jugular vein, cephalad to the affected hemithorax, an arterial line in the radial artery, cephalad to the affected hemithorax and a urinary catheter in the bladder, diurethrally.
Place the patient in a lateral supine position with the affected hemithorax facing upwards and apply bed movements to sufficiently open the intercostal spaces of the affected hemithorax. Recheck and confirm that the tracheostomy tube is functioning properly, with satisfactory lung closure of the affected hemithorax.
Αφαίρεση του σωλήνα θωρακικής παροχέτευσης, αποστείρωση του χειρουργικού πεδίου με διάλυμα ιωδιούχου ποβιδόνης και επικάλυψη γειτονικής περιοχής με άσηπτα οθόνια. Αρχικά δια της προϋπάρχουσας οπής του σωλήνα θωρακικής παροχέτευσης (που συνήθως έχει γίνει στην πρόσθια μασχαλιαία γραμμή, στο ύψος του 5ου μεσοπλευρίου) και τοποθέτηση trocar 11mm, διενεργείται θωρακοσκοπική διερεύνηση του πάσχοντος ημιθωρακίου με θωρακοσκοπική κάμερα 10mm και 30ο. Συνήθως ανευρίσκεται ελάχιστη πλευριτική συλλογή, η οποία παροχετεύεται τελείως με θωρακοσκοπική αναρρόφηση. Ακολούθως, υπό θωρακοσκοπική καθοδήγηση, διενεργούνται δύο νέες οπές 10mm, η μία στην πρόσθια μασχαλιαία γραμμή, στο ύψος του 7ου μεσοπλευρίου διαστήματος και η δεύτερη στη μέση ή οπίσθια, μασχαλιαία γραμμή, στο ύψος του 8ου μεσοπλευρίου διαστήματος. Η θωρακοσκοπική κάμερα μεταφέρεται στην οπή του 7ου μεσοπλευρίου διαστήματος και διενεργείται λεπτομερής θωρακοσκοπική διερεύνηση όλου του πάσχοντος ημιθωρακίου. Σε περιπτώσεις ύπαρξης συμφύσεων μεταξύ του σπλαχνικού και τοιχωματικού υπεζωκότα, αυτές λύονται θωρακοσκοπικά με ηλεκτροδιαθερμία, για την επίτευξη της πλήρους και ευχερούς επανέκπτυξης του πνεύμονα. Σε περιπτώσεις όπου υπάρχει εκτεταμένη παχυπλευρίτιδα, που παγίδευε μέρος ή λοβό ή ολόκληρο τον υποκείμενο πνεύμονα (trapped lung), διενεργείται πλήρης και σχολαστική αποφλοίωση. Μετά την πλήρη λοιπόν παροχέτευση της πλευριτικής συλλογής και της συμφυσιόλυσης ή/και αποφλοίωσης, διενεργείται πρόσκαιρη δοκιμασία επανέκπτυξης του πνεύμονα του πάσχοντος ημιθωρακίου, με άρση αποκλεισμού του σκέλους του δίαυλου τραχειοσωλήνα, που αερίζει τον πνεύμονα του πάσχοντος ημιθωρακίου. Εν συνεχεία, μετά την επιτυχή επανέκπτυξη του πνεύμονα, αποκλείεται και πάλι ο αερισμός του πνεύμονα του πάσχοντος ημιθωρακίου. Με την ινοπτική κάμερα στην αρχική της θέση, στο 5ο μεσοπλεύριο διάστημα κι υπό θωρακοσκοπική καθοδήγηση, γίνεται η τοποθέτηση σωλήνα θωρακικής παροχέτευσης 28Fr, δια της οπής του 7ου μεσοπλευρίου διαστήματος, του οποίου η τελική θέση βρίσκεται προσθίως της πνευμονικής πύλης και η άκρη του έφθανε μέχρι το θόλο του ημιθωρακίου. Αντιστοίχως, υπό θωρακοσκοπική καθοδήγηση, γίνεται η τοποθέτηση του 2ου σωλήνα θωρακικής παροχέτευσης 28Fr, δια της οπής του 8ου μεσοπλευρίου διαστήματος, του οποίου η τελική θέση βρίσκεται οπισθίως της πνευμονικής πύλης και η άκρη του μόλις ξεπερνά το ύψος της αζύγου ή ημιαζύγου φλέβας. Και οι δύο σωλήνες καθηλώνονται στο δέρμα με ράμμα 0 Prolene. Άρση αποκλεισμού του τραχειοσωλήνα διπλού αυλού. Η οπή στο 5ο μεσοπλεύριο διάστημα συρράβεται σε δύο στρώματα με Vicryl 2-0 και ενδοδερμική ραφή Vicryl 3-0.
The anterior tube high up towards the top of the thoracic cage serves for the inflow of the hyperthermal solution and the posterior tube lower down for the outflow of the hyperthermal solution (Figure 17). Connection of the above mentioned tubes to the extracorporeal circulation circuit (Performer HT by RanD S.A., Italy) (Figure 16). Re-sterilization of the surgical field with povidone iodide and covering it with dressing material and waterproof membrane (so that any fluid leakage is intraoperatively visible).
With the lung of the affected hemithorax in semi-expansion (so that the largest possible surface of the lung is in contact with the hyperthermic solution), the affected hemithorax is filled with 1-1. 6lt of hyperthermal solution (depending on the patient's body measurements and the hemodynamic burden due to the additional weight of the solution on the pericardial sac) and start circulating the solution at a rate of 1lt/min until an intrathoracic temperature of 41.5°C is reached. oC. On top of the circuit tubes there are electric thermometers that sublimate the temperature of the solution in the inlet and outlet tube and based on an algorithm the temperature of the solution is calculated intrathoracically. Usually the target of 41.5 oC is achieved in 8-12 min from the start of circulation). The solution is then enriched with 500 mg/m2 carboplatin (usual dose: 750 mg) and continue intra-abdominal circulation of the solution at the same rate and temperature for 45-60 min. The whole procedure is carried out under the supervision and guidance of the surgeon, while the operation of the extracorporeal circulation machine is the responsibility of Rand's specialized extracorporeal circulation technician.
Complete the procedure, drain all the solution from the affected hemithorax, disconnect the chest tubes from the extracorporeal circulation system and connect the chest tubes via a Y-connector to a Bülau device.

Image 16
Extracorporeal circulation machine Rand
Placing the patient in the supine position, gradual reduction of anaesthesia and muscle relaxation and waking the patient in the operating room. Intubation of the patient and transfer to the metanesthetic care room. Perform portable bedside radiography and transfer hemodynamically stable patient to the inpatient ward.
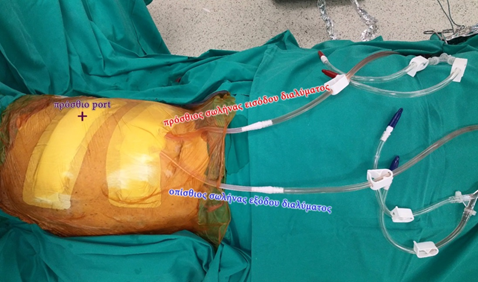
Image 17
Connection and adjustment of the extracorporeal hyperthermia circulation circuit

Surgical team
You can arrange an appointment with the doctor
In the morning the Thoracic Surgeon, Dr Athanasios Kleontas MD is at the Interbalkan Medical Center of Thessaloniki, while in the evening he is at his private office (73, Ermou St).
+30 2310 - 400000
Office 11, 2nd floor. Dec 1742
ATHANASIOS D. KLEONTAS
PATIENT VISITATION HOURS
Doctor is available (by mobile) 24 hours a day, 7 days a week.
You meet him only by appointment at his private office:
Monday to Friday : 18.00 - 21.00